About LHON
What is LHON?
Leber hereditary optic neuropathy (LHON) is an inherited form of mitochondrial disease resulting in rapid central vision loss.1,2
- LHON was the first human condition linked to a point mutation in the mitochondrial DNA (mtDNA). These mutations affect subunit genes of Complex I.3
- LHON presents with subacute, simultaneous or sequential, bilateral painless loss of central vision due to selective degeneration of the retinal ganglion cells (RGCs) and their axons.2 These cells are particularly vulnerable to mitochondrial dysfunction leading to optic nerve atrophy and loss of central vision.2
- Most patients with LHON end up legally blind.1


LHON is a mitochondrial disorder that results from point mutations in the mtDNA that encode components of respiratory Complex I (see figure below). Approximately 90% of the LHON cases come from three primary mtDNA mutations (m.3460G>A in MT-ND1, m.11778G>A in MT-ND4, and m.14484T>C in MT-ND6) that are maternally inherited.2,4
Although an mtDNA pathogenic mutation is an important factor, other mitochondrial, nuclear genetic, and environmental factors are also known to trigger LHON.5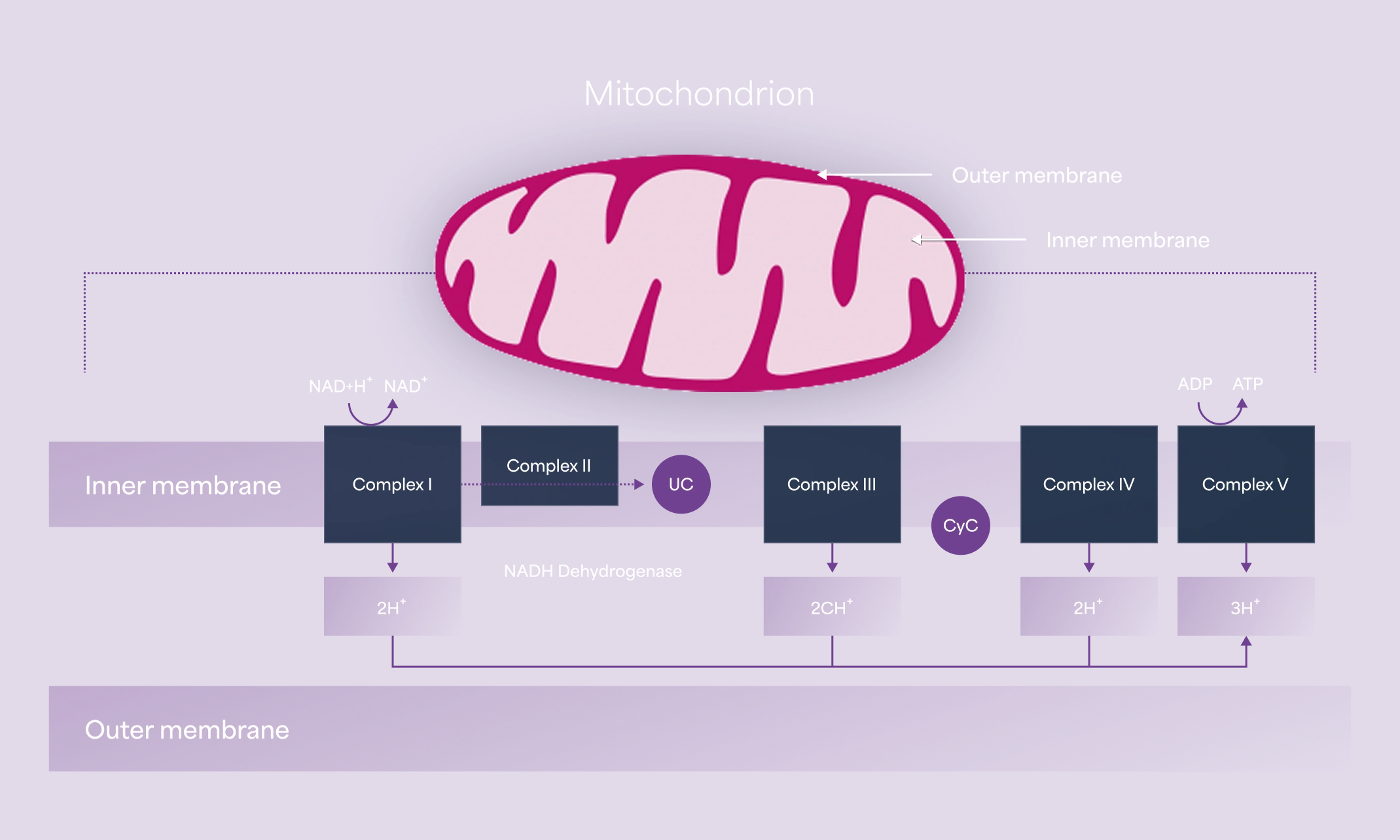
LHON affects predominantly men in their 20s or 30s and is most commonly seen in teenage boys and young men, which account for 80% of new cases.1,6
However, it can occur in individuals of all ages, including children and the elderly.1 Unlike men, women have no peak onset age.7 Men are three times more likely to be affected than women, but neither gender nor mutational status significantly influences the timing and severity of the initial visual loss.7 Recent evidence also suggests a protective role of estrogen and could explain LHON vision loss in menopausal women, given the declining levels of estrogen.8.png) Eliane (in green), Living with LHON
Eliane (in green), Living with LHON
.png) PAOLA AND GIANFRANCO, Living with LHON
PAOLA AND GIANFRANCO, Living with LHON
.png) SEBASTIAN, Living with LHON
SEBASTIAN, Living with LHON
What LHON eyesight looks like


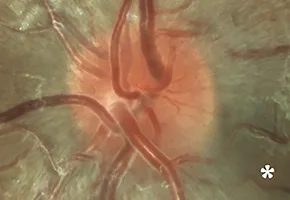
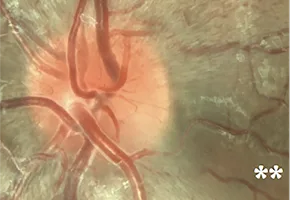
Optic disc images of 17-year-old boy with LHON from presymptomatic to chronic stage10
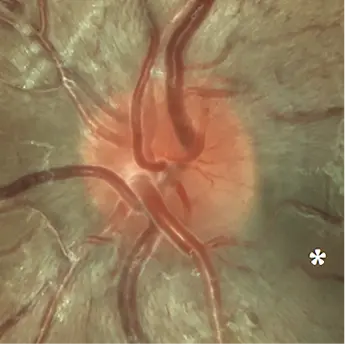

6 weeks before onset of visual loss: initial papillomacular bundle defect in the inferotemporal sector associated with diffuse hyperemia of the disc (*)10
4 weeks before onset: progression of the papillomacular bundle defect(**)10

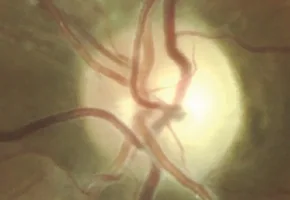
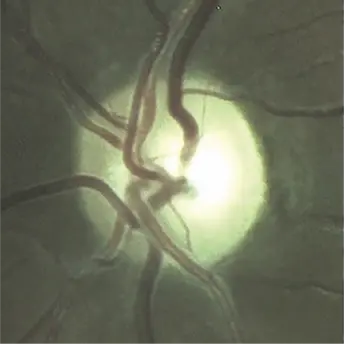

9 months after onset: optic atrophy with complete loss of papillomacular bundle10
17 months after onset: complete and severe optic atrophy10

Signs and symptoms
Bilateral, painless subacute visual failure that develops during young adult life11
- Disease progression is rapid in the acute phase, with visual acuity being diminished to ≤2/20 within 5 to 6 weeks of the onset of symptoms5
- Visual field testing by kinetic or static perimetry shows an enlarging dense central or centrocecal scotoma11
Disc hyperemia, edema of the peripapillary retinal nerve fiber layer, retinal telangiectasia, and increased vascular tortuosity11
- ~20% of affected individuals show no fundal abnormalities in the acute stage
Potential risk factorsand triggers
Risk factors:
Smoke in general (not just tobacco smoking)
Heavy alcohol consumption
Cyanide-containing products
Exposure to environmental factors, like pesticides and methanol, especially during the acute phase of visual loss
Medications with mitochondrial toxicity, including antibiotics such as ethambutol, chloramphenicol, linezolid, aminoglycosides, and antiretroviral drugs (for HIV)12
References
- Theodorou-Kanakari A, et al. Adv Ther. 2018;35(10):1510-1518.
- Kirches E. Curr Genomics. 2011;12(1):44-54.
- Carelli V, et al. Hum Mol Genet. 2017;26(R2):R139-R150.
- Carelli V, et al. European Ophthalmic Review. 2019;13(Suppl 2).
- Karaarslan C. Adv Ther. 2019;36(12):3299-3307.
- Stenton SL, et al. J Clin Invest. 2021;131(6):e138267.
- Poincenot L, et al. Ophthalmology. 2020;127(5):679-688.
- Asanad S, et al. J Curr Ophthalmol. 2019;31(3):251-253.
- Fraser JA, et al. Surv Ophthalmol. 2010;55(4):299-334.
- Atlas of Leber’s Hereditary Optic Neuropathy, 2018, MEDonline, ISBN: 978-90-828166-0-0
- Yu-Wai-Man P, et al. Leber Hereditary Optic Neuropathy. 2000. In: Adam MP, Bick S, Mirzaa GM, et al, eds. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2025. Updated March 2021.
- Sadun A, et al. Curr Treat Options Neurol. 2011;13(1):109-117.