Diagnosing LHON
Importance of early diagnosis
Leber hereditary optic neuropathy (LHON) is a rare, complex, and life-altering disease.1 The majority of patients will end up legally blind with a visual acuity of 20/200 or worse, which results in a significant detrimental impact on their quality of life.1,2
Diagnosis is often delayed because of the lack of disease awareness and the inability to differentiate LHON from other conditions with similar characteristics, especially in the absence of family history.3
Tests to confirm LHON
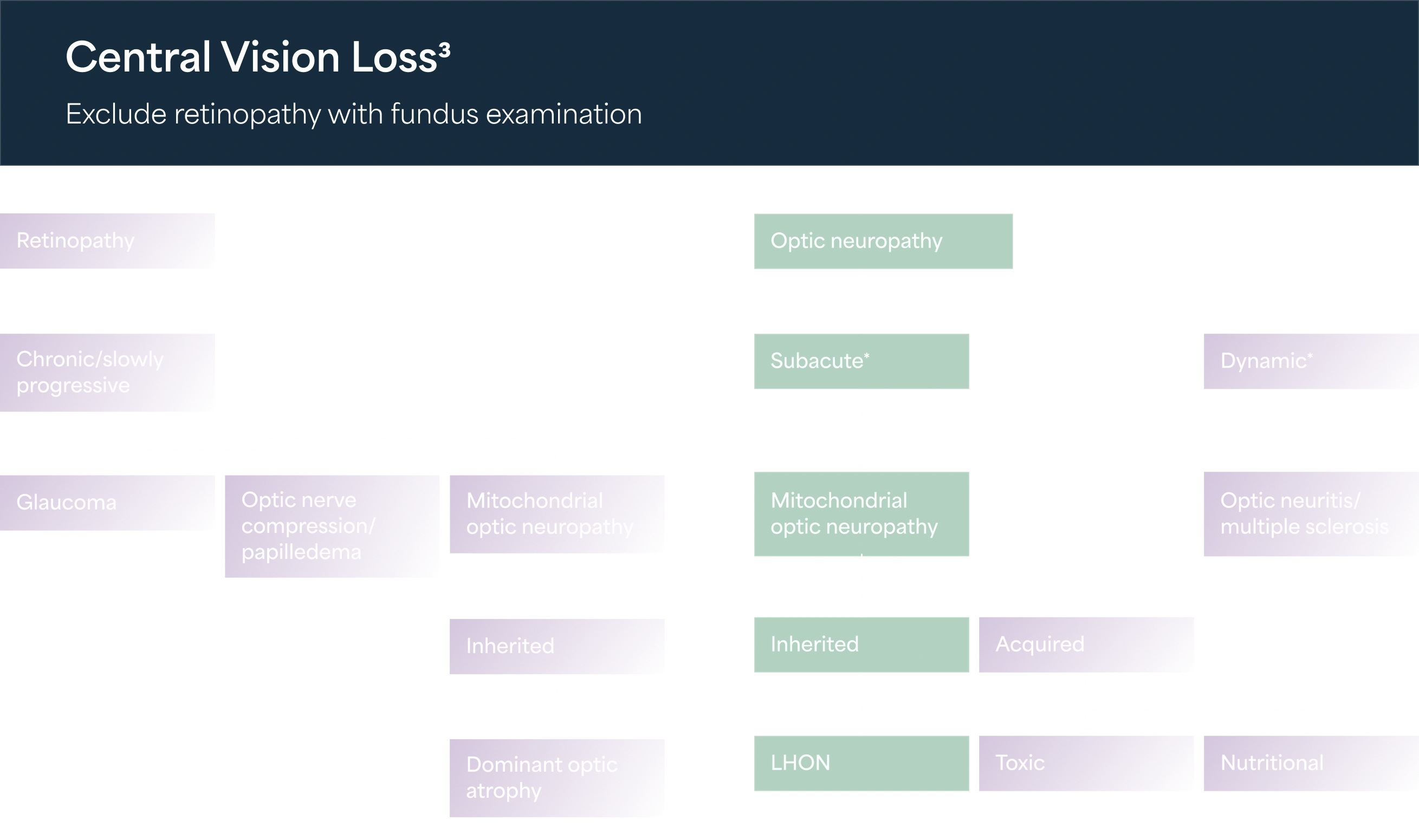
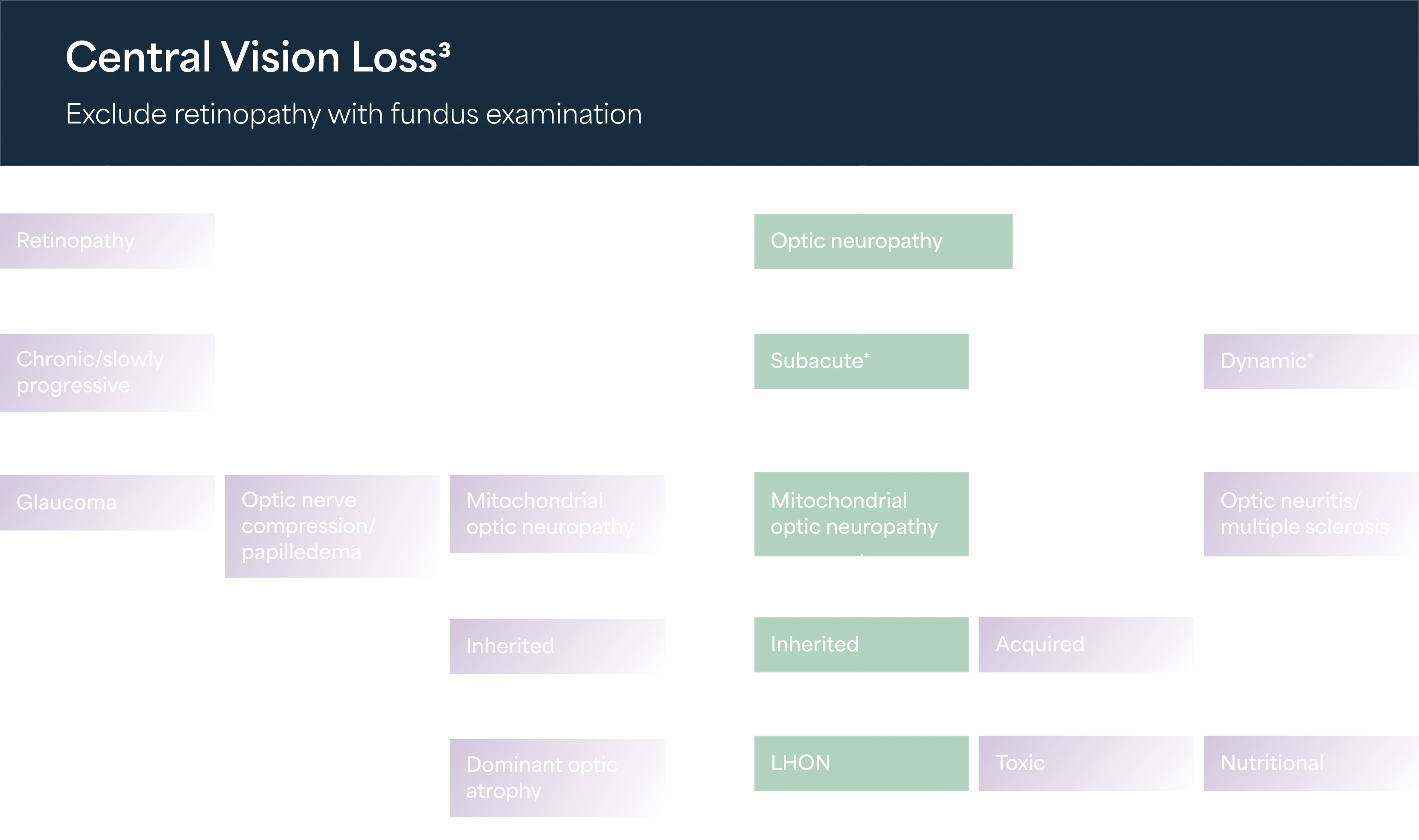
LHON is often mistaken for other medical conditions, such as a brain tumor, multiple sclerosis, and optic neuropathies, because of the nature of LHON symptoms that develop in one eye.4-7
In addition to symptoms such as visual loss, a patient with LHON can often provide a history of visual loss in family members along the maternal line.8




Some of the tests that help confirm LHON are:
This is an emerging non-invasive technique for evaluating ocular microvasculature. With this method, the peripapillary retinal and vascular circulation can be evaluated in three dimensions. Evaluation of vascular changes in LHON using OCTa may help us understand the pathophysiology of the disease, assess disease progression, and monitor the efficacy of treatment. OCTa is used to detect significant peripapillary microvascular changes over the disease course. In addition to the peripapillary region, OCTa studies have also provided evidence of pathology associated with the macular vasculature in different disease stages of LHON.
A mitochondrial DNA test (mtDNA test) traces a person’s mother-line using the DNA in their mitochondria. mtDNA is passed down by the mother unchanged to all her children. Both men and women can therefore take an mtDNA test.
LHON can usually be confirmed with an mtDNA blood test to reveal one of the three common mutations. Even if this test is negative, LHON may still be considered because approximately 5% of cases are not due to the three common LHON mutations. A complete mtDNA sequence analysis may be recommended if the clinical diagnosis of LHON remains a strong indication or if there’s evidence of maternal transmission of blindness.
DNA testing of primary LHON mutations is recommended in atypical presentations or in the absence of a clear family history of LHON.
Molecular genetic testing
Molecular genetic testing approaches can include gene-targeted testing methods such as targeted mtDNA analysis for pathogenic variants, multigene panel, and complete mtDNA sequencing.8
The first step is to perform a targeted analysis for the three common mtDNA pathogenic variants observed in ~90% of individuals with LHON.
This includes the mitochondrial genes that encode subunits of NA dehydrogenase (DH) (MT-ND1, MT-ND2, MT-ND3, MT-ND4, MT-ND4L, MT-ND5, and MT-ND6) known to cause LHON, and is most likely to identify the genetic cause of the condition at the most reasonable cost.
This is recommended if targeted testing and/or a multigene panel did not identify a pathogenic variant while clinical suspicion of LHON remains high.
 ACTOR PORTRAYAL
ACTOR PORTRAYAL

Diagnostic pathway
Without a known family history of LHON, the diagnosis usually requires a neuro-ophthalmological evaluation and blood testing for mtDNA assessment.3,8 It is essential to exclude other possible causes of vision loss and other system abnormalities.3
Due to its rare nature, diagnosis of LHON is a long process. It often takes weeks or months from the onset of symptoms to receiving a confirmed diagnosis.3
LHON patients are commonly misdiagnosed with optic neuritis and multiple sclerosis before they are properly diagnosed3
Referring your patient
Patients must get confirmation of an LHON diagnosis sooner to get timely help and management of their condition.3
If you encounter patients with sudden, unexplained, and painless vision loss, refer them to any of the following without further delay.
A neuro-ophthalmologist
A specialist LHON clinic
 ACTOR PORTRAYAL
ACTOR PORTRAYAL

References
- Theodorou-Kanakari A, et al. Adv Ther. 2018;35(10):1510-1518.
- Kirkman MA, et al. Invest Ophthalmol Vis Sci. 2009;50(7):3112-3115.
- Carelli V, et al. European Ophthalmic Review. 2019;13(Suppl 2).
- Meyersen C, et al. Clin Ophthalmol. 2015;9:1165-1176.
- Yu-Wai-Man P, et al. Prog Retin Eye Res. 2011;30(2):81-114.
- Fraser JA, et al. Surv Ophthalmol. 2010;55(4):299-334.
- Pfeffer G, et al. Neurology. 2013;81(24):2073-2081.
- Yu-Wai-Man P, et al. Leber Hereditary Optic Neuropathy. 2000. In: Adam MP, Bick S, Mirzaa GM, et al, eds. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2025. Updated March 2021.
- Sadun A, et al. Curr Treat Options Neurol. 2011;13(1):109-117.
- Kızıltunç PB, et al. Turk J Ophthalmol. 2020;50(5):313-316.
- Asanad S, et al. Ther Adv Ophthalmol. 2020;12:2515841420950508.
- International Society of Genetic Genealogy Wiki. Accessed: January 7, 2026. https://isogg.org/wiki/Mitochondrial_DNA_tests
- Yu-Wai-Man P, et al. J Med Genet. 2002;39(3):162-169.
- Stenton SL, et al. J Clin Invest. 2021;131(6):e138267.